Real Time Prior Authorization: Closing the Gap at the Point of Care
Lynn Kha, Tensility Intern and MBA Candidate at Northwestern Kellogg School of Management
Wayne Boulais and Armando Pauker, Managing Directors, Tensility Venture Partners
Introduction
Prior authorization, the process by which insurance companies approve or deny treatment, is one of the most visible sources of frustration in healthcare today. AI tools have emerged as one potential way to reduce this burden, but these exist as point solutions. Even as tools get smarter and workflows get faster, the core disconnect remains: the clinical decision and the payer approval process still happen separately, leading to delays and high administration costs. This blog explores a different approach: bringing prior auth intelligence and decision-making directly into the clinical encounter or office visit. We also examine why technology alone cannot solve this critical problem. We identify barriers such as liability, industry coordination, and preserving physician decision-making that any solution should address.
The Current Landscape
Prior authorization requires healthcare providers to obtain approval from insurance companies before delivering certain treatments, procedures, or medications to patients. It delays care, creates rework, triggers appeals and peer-to-peer calls, and forces physicians into clerical roles when they should be focused on patients.
Software automation is already being deployed today in clinical settings. AI-powered tools are making a meaningful dent in the administrative work that pulls clinicians away from patient care. From automating back-office workflows to supporting real-time documentation, a growing set of tools is becoming popular.
● Back-Office Prior Auth Automation: These tools automate the prior auth submission and tracking process, gathering clinical documentation, submitting requests, monitoring payer responses, and escalating when needed. Cohere Health is a leading example, purpose-built to streamline prior auth for either health systems or payers.
● Scribing and Documentation Tools: These tools listen to patient visits in real time, drafting clinical notes, suggesting billing codes, and triggering downstream revenue workflows automatically. Abridge, for example, helps clinicians reclaim time spent on documentation after every office visit.
● Clinical Support Tools: These tools work inside the Electronic Health Record (EHR) to surface relevant patient history, flag potential gaps in care, and draft care plans for clinician review. Regard, for example, is designed to give physicians a clearer picture of each patient's longitudinal record at the point of care
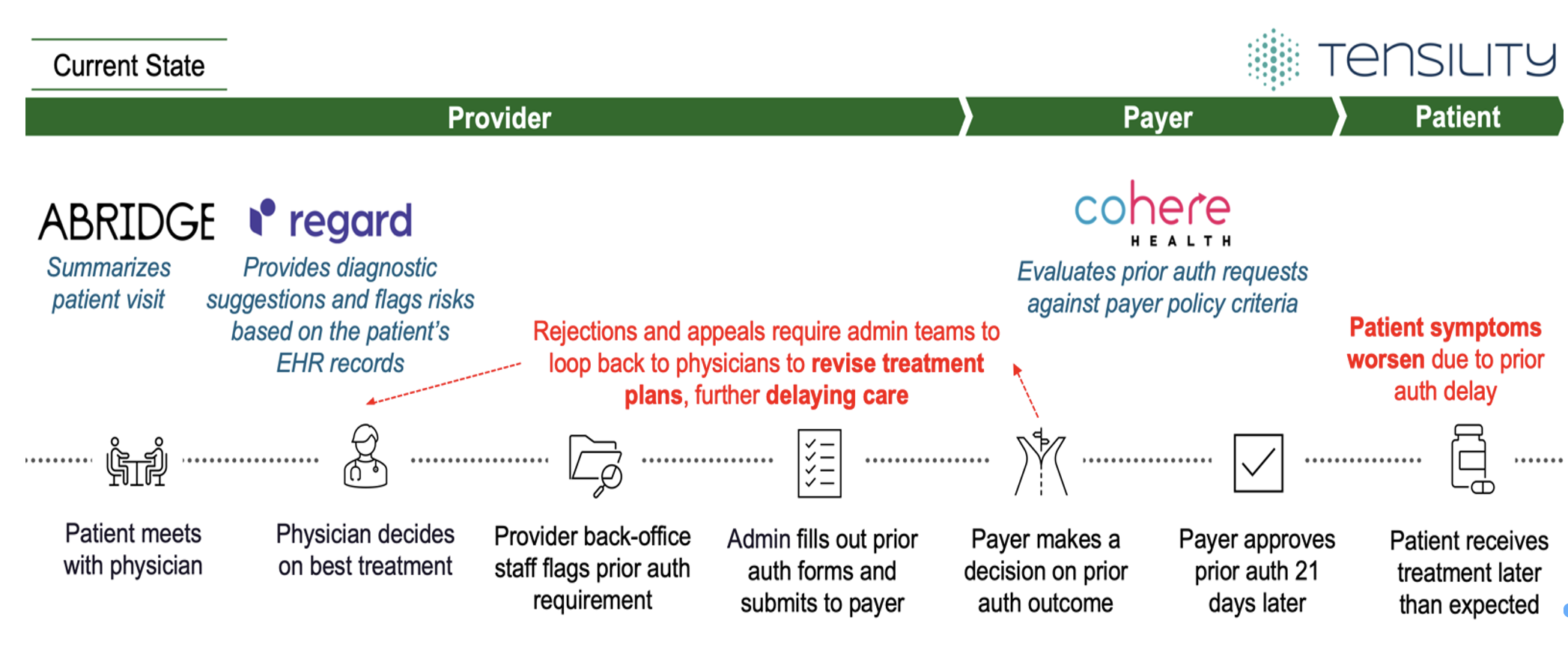
Even with real gains from automation, prior authorization remains a problem. While current solutions help the clinician’s workload, they do not automate the critical prior authorization process because they focus on the steps either before or after prior authorization is initiated, not in real time during the clinical decision itself. Figure 1 emphasizes this gap: clinicians still face denials they could not see coming, patients still wait longer than they should, admin teams still spend their days chasing paperwork, and treatment plans are still getting revised after the fact. Tools like Cohere Health, as effective as they are, operate downstream from the clinical encounter, supporting back-office and utilization management teams rather than the clinician making treatment decisions. That makes them well suited for processing prior auth requests efficiently, but they have no ability to inform the decision at the moment care is being planned. The clinical encounter and the payer's decision remain two separate processes, with patients and clinicians left to deal with the gap between them.
Figure 1. Treatment is potentially delayed due to prior authorization requirements
Proposed Solution: Real-Time Prior Auth at Point of Care
We propose that the industry think about bringing prior auth intelligence into the clinical encounter while care is being delivered, not after the fact. In Figure 2, we propose an agentic layer across the entire workflow, listening to the patient visit, pulling in longitudinal history from the EHR, and running payer logic in real time to surface which treatment paths are most likely to get approved. Instead of finding out days later that a plan was denied, the clinician gets that signal immediately and can adjust the treatment plan with confidence. The result is fewer rejections, less rework, and patients who get access to the care they need without unnecessary delays. Additionally, this approach addresses overutilization, a key concern from the payer perspective. By surfacing payer policies and clinical best practices in real time, the system helps ensure that treatment recommendations align with established guidelines. Rather than relying on denials after the fact to discourage overutilization, the system provides proactive guidance that benefits both appropriate care delivery and cost management. This solution shifts the entire prior auth process from reactive cleanup to proactive, real time decision support.
Figure 2. Treatment is approved quickly, enabling timely access to care
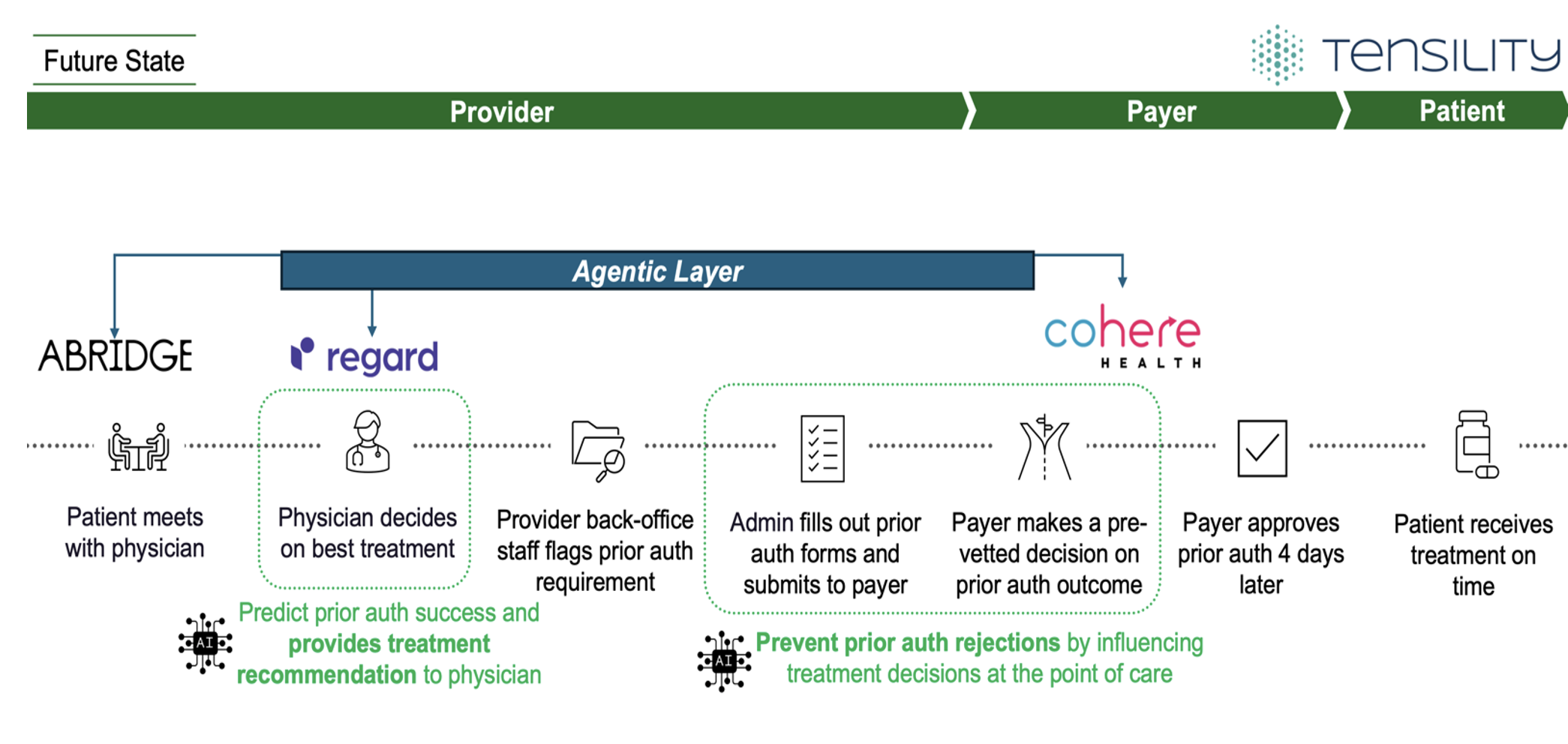
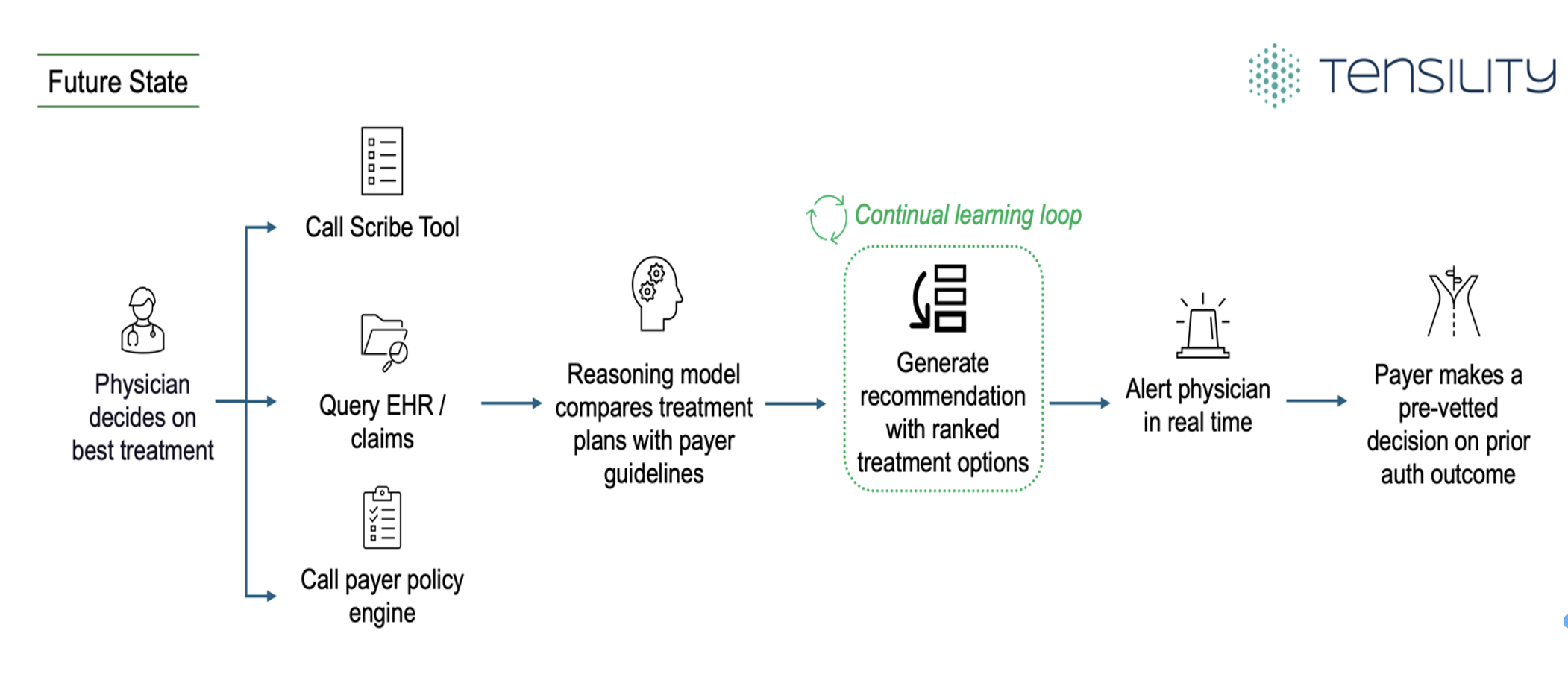
Figure 3 highlights three distinct capabilities required to formulate this agentic layer:
Call scribe tool: Captures the real-time conversation and drafts diagnosis notes as the visit unfolds
Query EHR and claims data: Pulls the patient's full history, including prior treatments, allergies, diagnoses, etc.
Query payer policy engine: Retrieves current insurance guidelines relevant to that patient, coverage details, and step therapy requirements
With all three inputs, a reasoning model with learning capabilities compares potential treatment plans against payer guidelines and historical approval patterns, then generates ranked treatment options with predicted approval scores. The clinician sees these recommendations pushed directly into the EHR interface in real time. Every decision, every approval, and every denial feeds back into the model, creating a continual learning loop that makes the recommendations sharper and more accurate over time. The more the system is used, the better it gets at predicting what will get approved and ultimately improve timely patient care.
Figure 3. Agentic Layer Deep Dive
Barriers Beyond the Technology
This vision is technically feasible. However, technology alone cannot solve this problem. US healthcare solutions must take into consideration real barriers including liability, industry coordination, and preserving physician decision-making along with careful policy and compliance considerations.
The most significant legal issue centers around the theory of the “practice of medicine” and who bears responsibility for the consequences of a prescribed treatment. In the US, only those who hold a valid license from a state’s medical board are permitted to practice medicine. This precludes insurance companies from practicing medicine. However, the more directly a payer’s coverage decisions influence what gets prescribed, the harder it is to claim the payer is not driving the decision and therefore practicing medicine. If an AI agent flags that a CT scan is unlikely to be approved and the physician pivots to a different option, was that the doctor's clinical judgment or the insurance company's policy? When payers effectively dictate treatment decisions, even indirectly through an AI agent, they risk crossing into the practice of medicine. A payer will take legal and liability risks if they are dictating treatment options, and the consequences of getting it wrong could be significant in terms of cost and patient outcomes.
Additionally, a growing automation arms race complicates this further. Payers are deploying AI bots that require more information from providers before processing prior auth requests. What used to take a provider staff member five minutes to fill out the required forms now takes fifteen to thirty minutes because they must manually load more data into the payer's system. Health systems are responding by deploying their own AI tools to keep up. The result is two automated systems negotiating with each other while the clinicians and staff are caught in the middle, losing visibility into what is being decided. Each side is acting in its own best interest, but the compounding inefficiency is unsustainable.
Any effective solution would need to go beyond an AI technical solution and address both problems. The provider should own and manage our proposed system, since this leads to faster treatment for patients while enabling faster reimbursement and less administrative rework, but the payer needs to cooperate. The agentic layer would integrate with the payer's systems, potentially handling the back-and-forth to make sure all required information is submitted correctly up front. But even with perfect technical integration, the legal question remains. The agent cannot make the clinical decision. It can inform, recommend, and streamline, but the final call has to stay with the physician. Otherwise, liability shifts, and the entire process falls apart.
Conclusion
Building a better prior auth system is not just about picking the right agentic technology or deploying smarter workflows. It requires thoughtful consideration of factors that span beyond LLMs, APIs and technology. An optimal design ensures that the AI and insurance company policies do not make treatment decisions but instead supports physicians in making them. Coordination is needed across payers and providers who are currently locked in an automation arms race. Lastly, a shared commitment is needed to make sure that technology simplifies the system to improve patient care rather than automating the dysfunction that already exists. The tech and AI components are ready. The question is whether the industry is willing to do the harder work of aligning the various stakeholders and incentives, clarifying liability, and building solutions that address the prior authorization bottleneck. If it can, prior authorization could shift from being one of healthcare's biggest frustrations to one of its most seamless and efficient processes.